Oesophago-Gastro-Duodenoscopy

Colonoscopy

Enteroscopy of the small bowel

Capsule Endoscopy of the small bowel

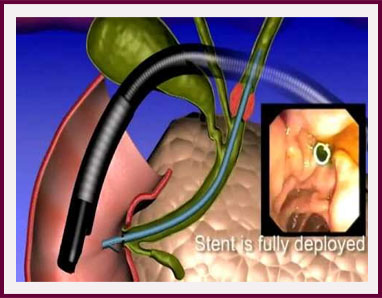
Endoscopic Retrograde Cholangio-Pancreatography (ERCP)

Liver Biopsy

Dilatation of oesophageal strictures

Insertion of oesophageal stents

Injection sclerotherapy and band-ligation of oesophageal varices
Insertion of percutaneous endoscopic gastrostomy (PEG) feeding tube

Haemostasis (excluding oesophageal varices which is discussed elsewhere)

Laser or Argon-Plasma Beam re-canalisation

Removal of polyps

Haemostasis (stopping bleeding) of bleeding lesions

Insertion of stents

Laser re-canalisation of inoperable colon cancer

Treatment of haemorrhoids

Sphincterotomy and extraction of gallstones from the bile ducts

Stenting of the bile ducts or pancreatic duct

Conversion of external-internal biliary stent to endoscopic stent ('rendezvous procedure')